
| Product | Catalog No | Product Insert |
|---|---|---|
| gASCA IgG | S701100 | click for pdf |
| ALCA IgG | L703011 | click for pdf |
| ACCA IgA | C702100 | click for pdf |
| AMCA IgG | M704100 | click for pdf |
| Anti-C IgA | AC706100 | click for pdf |
| Anti-L IgA | AL707100 | click for pdf |
The bacterial intestinal microbiota plays major roles in human physiology and IBD. Recent studies have
been shown to characterise the faecal fungal microbiota in patients with IBD.
9, 10.
The IBDX research kits are an excellent tool to study fungal macrobiota dysbiosis in IBD. As shown in the figures below, two dominant fungal species microbiata are associated with IBD. Saccharmoyces cerevisiae (IBDX gASCA) and Candida albicans.
C. albicans glycans are distributed into 40% glucans (polymers of [1]alpha-1,3 glucose [i.e. ALCA] and -1,6-glucose [i.e. Anti-L]), 2 to 4% chitin [i.e. ACCA/Anti-C], and 30% mannose chains [i.e. AMCA].
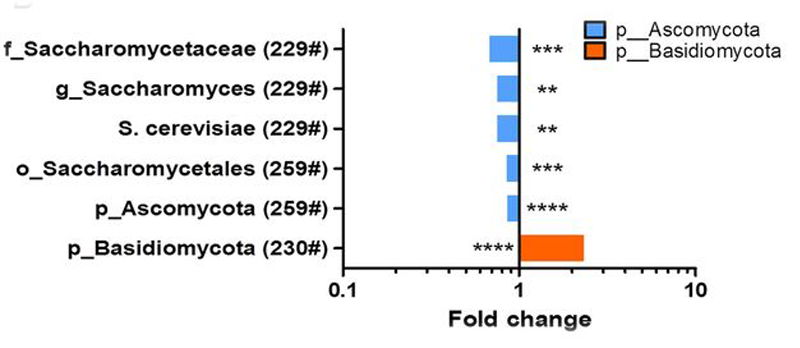
Fungal microbiome associated with IBD. Differences in abundance are shown for the fungal taxa detected using ITS2 sequencing and a multivariate statistical approach
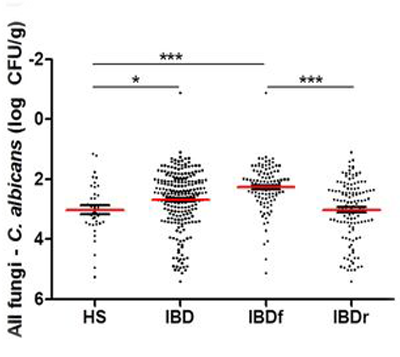
Absolute C. albicans abundance in the faecal microbiota quantified using qRT-PCR (mean±SEM).
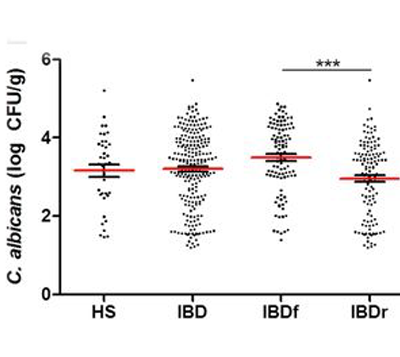
Relative proportion of Candida albicans calculated by subtracting the log number of C. albicans from the log number of all fungi.
*adopted from: Sokol et al Gut 2016, 0:1
Multiple studies have been show correlation between biomarkers seroreactivity and innate immunity genes.2, 3, 4, 5, 8,
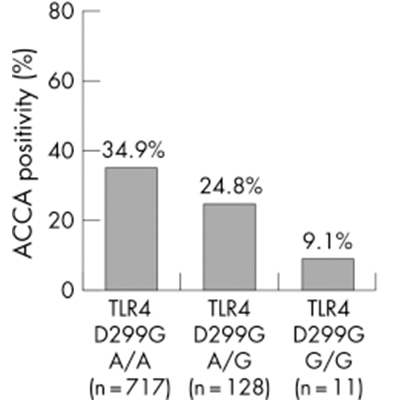
Anti‐chitobioside antibodies (ACCA) and Toll‐like receptor (TLR) 4 D299G, overall p value less than 0.026.
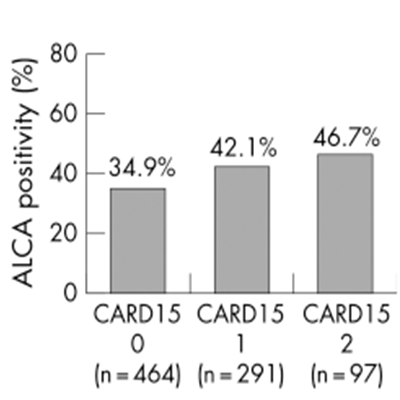
anti‐laminaribioside antibodies (ALCA) and CARD15, overall p value 0.04.
*adopted from: Henckaerts et al Gut Online 2007, 1536-1542
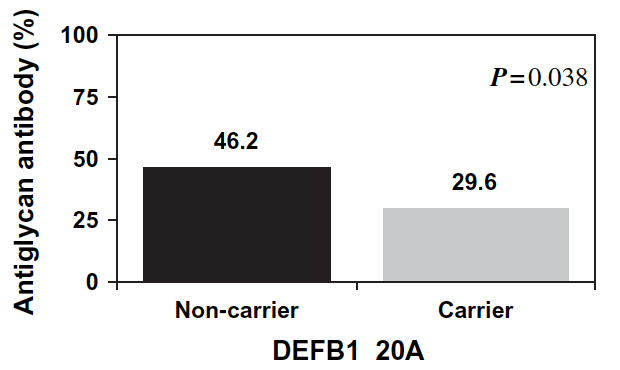
Anti-Glycan antibody positivity in patients with
Crohn’s disease due to DEFB1 genotypes.
*adopted from: Lakatos et al. Tissue Antigens, 2008 71(6), 552-559.
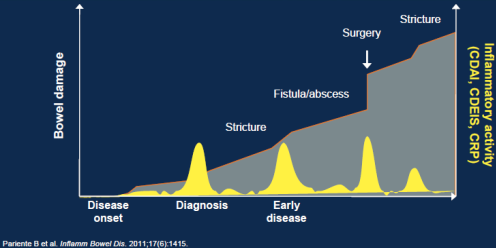
Inflammatory Activity and Progression of Bowel Damage in a Theoretical Patient with CD.
Studies have shown correlation between the number of positive serological IBDX markers and Crohn's Disease behavior and abdominal surgery1, 2, 3, 6, 9, 13, 18 including pediatric population 14, 16
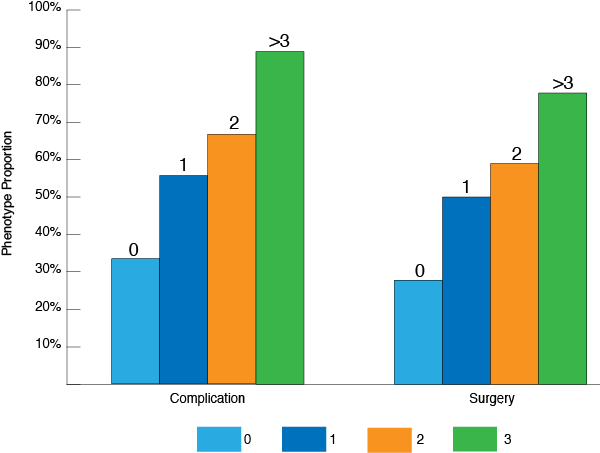
number of positive serological markers
*adopted from Reider et. al. 2010 IBD 16 (2) 263-274
*adopted from Rieder et al., Inflamm Bowel Dis 2010 16 (8), 1367-1375.
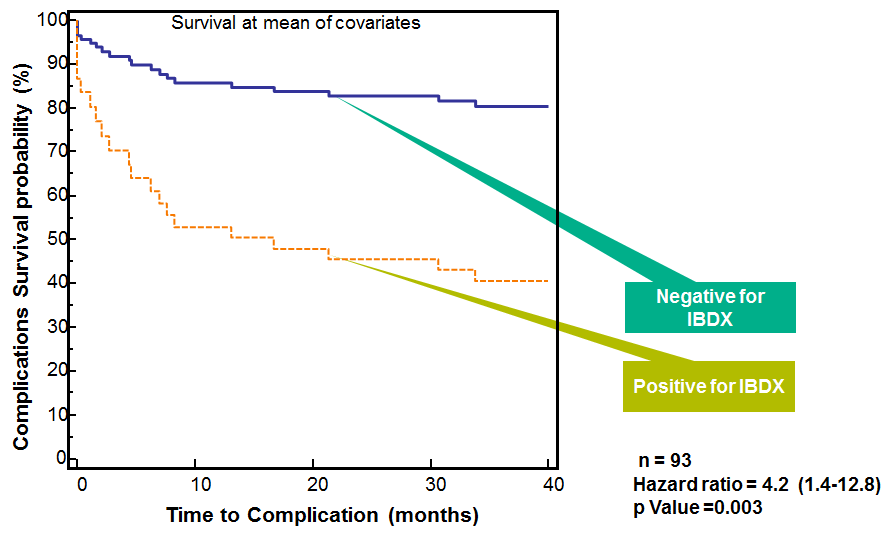
Prospective study demonstrated that Chron’s disease patients positive for at least two IBDX antibodies are at a higher risk to progress faster10
Studies have shown that the IBDX ACCA, AMCA and Anti-L can predict Ulcerative Colitis patients who went through ilial pouch-anal anastomis (IPAA) surgery and developed pouchitis 5, 7, 17
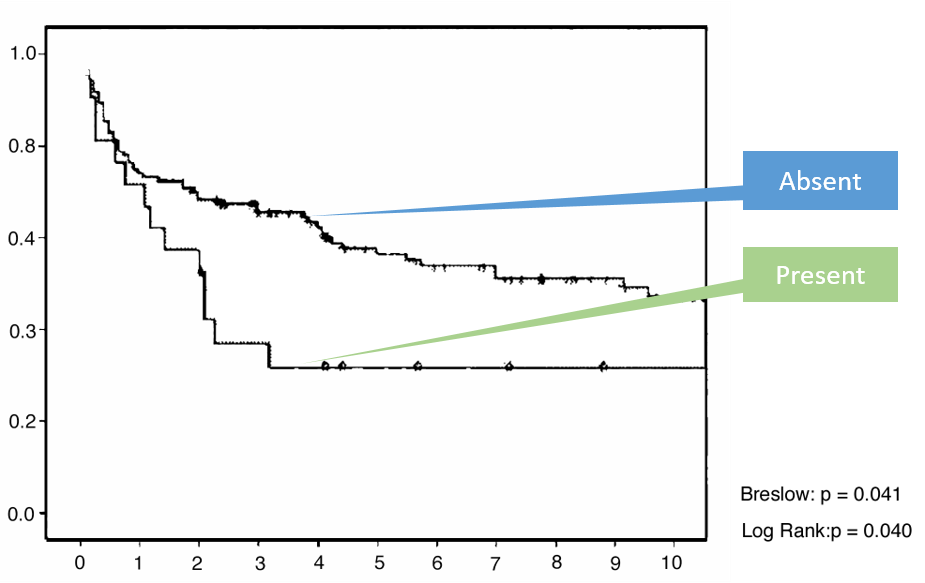

* adopted from Ferrante et al., JCC 2008 (2), 142-151.